Reproductive Aspects of Acute Appendicitis
 "Reproductive Aspects of Acute Appendicitis")
Introduction
Appendicitis most often occurs between the ages of 10 19 years, with an incidence of between 19-28 per 10,000 before the age of 14 years. Less than 7 per 10,000 children present with appendicitis before the age of 4 years & less than 5% of presentations with appendicitis occur before the age of 5 years.
Causation
In tropical climates the cause is often a parasitic worm (pinworm or roundworm) causing obstruction whereas in temperate climates the cause of obstruction of the appendix is more likely to be mechanical twisting or lymphoid hyperplasia associated with viruses such as adenovirus and rubeola or an endoluminal faecolith or undigested food. Periumbilical pain signifies appendiceal colic associated with the obstruction.
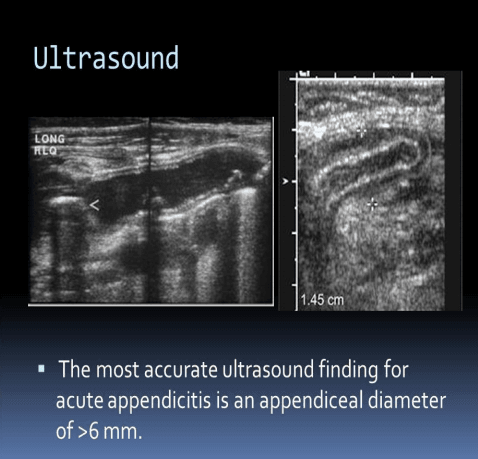
As part of the obstruction the lumen of the appendix increases in diameter and this is the basis of the ultrasonic diagnosis of appendicitis: the diameter exceeds 6 mm.
The proliferation of bacteria results in penetration of the wall of the appendix which becomes inflamed and gangrenous. When the pain moves to the right iliac fossa and becomes constant then inflammation of the appendix is underway. Perforation occurs rarely in the first 12 hours of symptoms but is more likely with time thereafter, becoming common after 72 hours.
Generalized peritonitis develops if the infection is not contained by bowel loops and omentum.
Delays in Diagnosis in Young Girls
Prior to rupture there appears to be no effect of appendicitis on tubal function however when the diagnosis is delayed and perforation has already occurred at the time of surgery tubal damage is increased (Relative Risk =4.8;95% CI =1.5-
14.9).
Future Risk of Ectopic Pregnancy
There appears to be a significantly increased risk of ectopic pregnancy in women who have appendicitis. In one study Elraiyah et al found the risk to be (OR=1.78,95% CI=1.46-2.16). A study by Fernandez et al found a similar increase in the risk of ectopic (RR= 2.2 ;95 percent CI: 1.5-3.2 ) but there appeared to be no difference in the ectopic rate between ruptured and unruptured appendices.
Appendicitis in Pregnancy
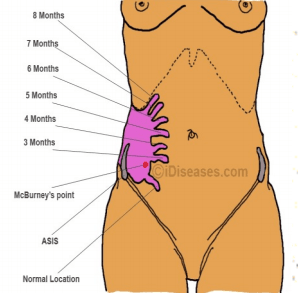
In a classic case of appendicitis in pregnancy Tthe pain is periumbilical & colicky initially and then migrates to the right lower quadrant as a constant pain as the inflammatory process progresses Anorexia, nausea and vomiting, if present, follow the onset of pain. Fever up to 38.3ºC and leukocytosis develop later. Many patients have a nonclassical presentation, with symptoms such as heartburn, bowel irregularity, flatulence, malaise, or diarrhea. If the appendix is retrocecal, patients often complain of a dull ache in the right lower quadrant rather than localized tenderness. Rectal or vaginal examination in such patients is more likely to elicit pain than abdominal examination. A pelvic appendix can cause tenderness below McBurney's point. The most common symptom of appendicitis, ie, right lower quadrant pain, occurs close to McBurney's point in the majority of pregnant women, regardless of the stage of pregnancy however, the location of the appendix migrates a few centimeters cephalad with the enlarging uterus, so in the third trimester, pain may localize to the mid or even the upper right side of the abdomen (see figures)
Investigations
- WCC. Approximately 80 percent of nonpregnant patients with appendicitis have a preoperative leukocytosis (white cells >10,000 cells/microL) and a left shift in the differential. However, mild leukocytosis can be a normal finding in pregnant women: the total leukocyte count may be as high as 16,900 cell/microL in the third trimester.
- Ultrasound of Appendix. The initial modality of choice for diagnostic imaging of the appendix in pregnancy is graded compression ultrasonography. The clinical diagnosis of suspected appendicitis is supported by identification of a non-compressible blind-ended tubular structure in the right lower quadrant with a maximal diameter greater than 6 mm.
- MRI .For pregnant women whose ultrasound examination is inconclusive for appendicitis, magnetic resonance imaging (MRI) is the preferred next test as it avoids the ionizing radiation of computed tomography and appears to be cost-effective
Obstetric Consequences of Acute Appendicitis in Pregnancy
The main complication is threatened preterm labour. In one study contractions occurred in 83% of all appendicitis patients in pregnancy >24 weeks with 13% exhibiting changes in cervical dilatation. The advent of laparoscopic appendicectomy has encouraged earlier diagnosis and treatment. Delayed diagnosis can have dire adverse effects on the fetus due to prolonged sepsis.
Further Reading
- Mueller BA et al.Appendicectomy and the risk of tubal infertility. NEJM 1986.315:1506-1508
- Elraiyah T et al. The effect of appendectomy in future tubal infertility and ectopic pregnancy: a systematic review and meta-analysis. J Surg Res 2014.192(2)368-374
- Fernandez et al. Appendectomy, a risk factor for ectopic pregnancy La Presse Medicale 1992 21(39):1859-1861.
- Williams R, Shaw J Ultrasound scanning in the diagnosis of acute appendicitis in pregnancy. Emerg Med J. 2007 May;24(5):359-60
| Tags:UltrasoundObstetrcisOther |