Inherited Risks of Gynaecological Cancer
 "Inherited Risks of Gynaecological Cancer")
Recently I saw a woman with a BRCA gene mutation who had recently had both breasts removed and was now being urged to have both ovaries removed, she was 39 years of age.
Understandably she was considerably anxious about the prospect of losing most physical vestiges of her femininity. She was keen to know how much risk she would incur of ovarian cancer if she deferred her bilateral oophorectomy until she reached 45 years of age.
Hereditary Breast and Ovarian Cancer Syndrome (HBOC).
The BRCA genes 1& 2 are located on chromosomes 17 and 13 respectively. Their normal role is in tumour suppression by recognising and repairing DNA damage. They are autosomal dominant.
In mutations which impair that function there are increased risks of breast and ovarian cancer:
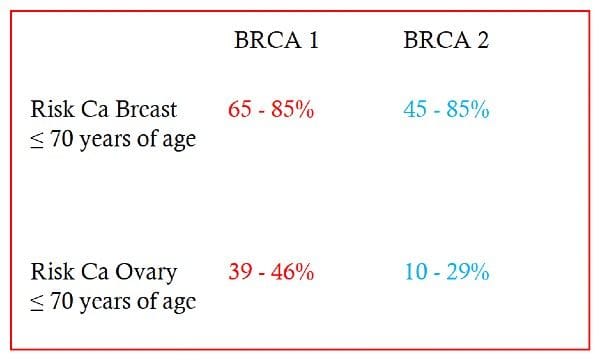
The current recommendations for removal of tubes and ovaries (RRSO) with BRCA mutations are as follows:
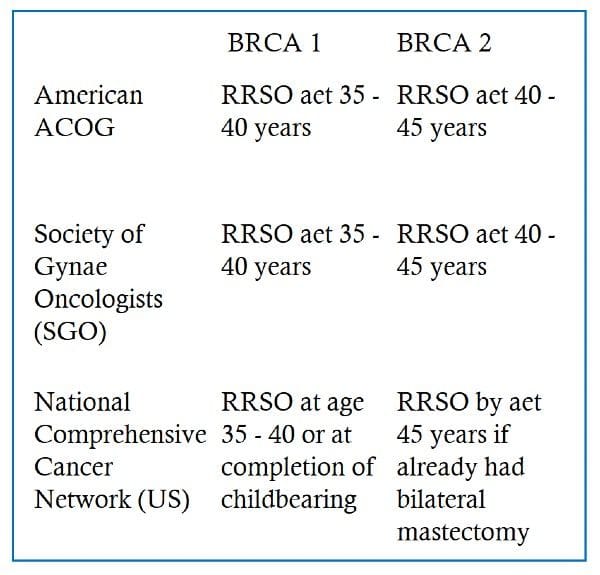
In a paper by Kotsopoulos et al in 2018 the cumulative risk was 0.55% to age 35 for BRCA1 mutation carriers and 0.56% to age 45 for BRCA2 mutation carriers. The authors recommend bilateral salpingo-oophorectomy before age 40, but ideally by age 35, for women with a BRCA1 mutation and by age 45 for those with a BRCA2 mutation to maximize prevention and to minimize adverse effects. The major problem with ovarian conservation is the weakness of current methods of detecting ovarian cancer These include serum ovarian tumour markers such as CA125,CA19.9,HEA and ROMA even when combined with ultrasound. Both the ACOG and the SGO emphasise that patients should be informed about lack of evidence supporting routine screening and that routine screening.
Lynch Syndrome
Lynch syndrome is an autosomal dominant condition closely associated with colorectal, endometrial and ovarian cancer .The genetic mutation responsible involves a defect in DNA mismatch repair (MMR) similar to BRCA genes. It has high penetrance Endometrial cancer is often the first cancer to be diagnosed in women with Lynch syndrome. It is thought that approximately 3% of women with endometrial cancer have Lynch syndrome but the vast majority are unaware.
Overall it is thought that 1/440 individuals have Lynch syndrome which would make it the most common inherited cancer syndrome. In Denmark the incidence is 1:278 individuals.
Of those patients with colon cancer the incidence of Lynch syndrome is again approximately 3%.
Screening for Lynch Syndrome.
The National Institute of Clinical Excellence recommends that where possible women with endometrial cancer especially those under the age of 70 years should be screened for Lynch syndrome because of its additional risks of colorectal and ovarian cancers.
Screening based on family history , although important, has a very low sensitivity.
Testing is predominantly tumour-based and involves immunohistochemistry for the MMR (mismatch repair) deficiency which is associated with a lack of MMR proteins in the tumour such as the endometrium. This has a sensitivity of 80-100 % and a specificity of 60-80%. An alternate strategy with similarly high sensitivity and specificity is based on DNA micro-satellite instability.
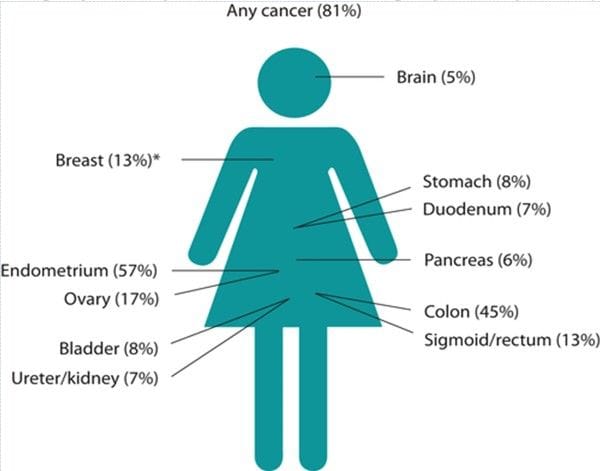
The risks of gynaecological cancer in Lynch syndrome are shown below:

Recommendations for Lynch syndrome prophylactic strategies
The lifetime risk of gynaecological cancer is sufficiently high to offer total hysterectomy and bilateral salpingooophorectomy for women with Lynch syndrome who have completed childbearing.
However the survival benefit achieved by riskreducing surgery is minimal because Lynch syndromeassociated endometrial and ovarian cancers have a good prognosis.
Aspirin:
Low dose aspirin reduces the risk of endometrial cancer in obese women and taking aspirin reduces the risk of all cancer types in Lynch syndrome carriers.
Hormonal:
The oral contraceptive pill reduces the risk of sporadic endometrial and ovarian cancer as well as BRCA-related ovarian cancer so it may have a useful role especially in younger women. The Mirena device may have a similar beneficial role.
Lifestyle changes:
Obesity, Type 2 diabetes and Tamoxifen exposure increase the risk of endometrial cancer so these can be modified.
Further Reading:
Kotsopoulos J, Gronwald J, Karlan B, Rosen B et al Hereditary Ovarian Cancer Clinical Study Group. Age-specific ovarian cancer risks among women with a BRCA1 or BRCA2 mutation. Gynecol Oncol. 2018 Jul;150(1):85-91. Ryan NAJ, McMahon RFT et al Lynch Syndrome for the gynaecologist The Obstetrician and Gynaecologist (RCOG) 2021 23(1)9-20
| Tags:OvariesOther |