Medico- Legal Aspects of Shoulder Dystocia
An increasing number of recent requests for expert evidence seem to involve claims for brachial plexus palsy in babies as a result of shoulder dystocia. The definitions are as follows:
1. Shoulder Dystocia: (incidence 0.5-1.5% of deliveries
a.Prolonged Head to Body Delivery Time >60 seconds
b. Resnik (1980) : Condition requiring special manoeuvres after failure to deliver the shoulders with downward traction
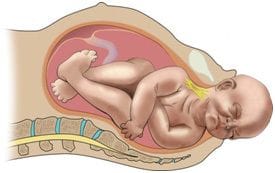
c. Arrest of spontaneous delivery due to impaction of the anterior shoulder against the symphysis pubis
2. Brachial Plexus Palsy Incidence 4-16% of cases of shoulder dystocia. However it can occur in up to 50% of cases without shoulder dystocia.
a. The brachial plexus is a network of spinal nerves that originates in the back of the neck, extends through the axilla (armpit), and gives rise to nerves to the upper limb (arm). The brachial plexus is formed by the union of portions of the fifth through eighth cervical nerves and the first thoracic nerve, all of which come from the spinal cord.
Erb’s Palsy: paralysis affecting the muscles of the upper arm and shoulder that is caused by an injury during birth to the upper part of the brachial plexus.
- C5 and C6 injury (Erb's palsy) accounts for approximately 50 percent of cases. Weakness involves the deltoid and infraspinatus muscles (mainly C5) and biceps (mainly C6). As a result, the upper arm is adducted and internally rotated, and the forearm is extended, while hand and wrist movement are preserved
- C5 to C7 injury (Erb's palsy plus) accounts for approximately 35 percent of cases and manifests as adduction and internal rotation of the arm, extension and pronation of the forearm, and flexion of the wrists and fingers, sometimes referred to as the "waiter's tip" posture

- 50% occur in babies <4kg
- The cause of neonatal brachial plexus palsy has been attributed to obstetric-related lateral traction on the fetal head, typically when shoulder dystocia impedes delivery. However, many cases of brachial plexus injury are not due to shoulder dystocia or excessive force by the provider. These cases where no shoulder dystocia has occurred probably happen as the fetal shoulder is damaged by uterine propulsive forces themselves against a resistant fetal shoulder.
- Neonatal brachial plexus palsy has been observed after delivery by cesarean section
Risk Factors for Shoulder Dystocia
- Macrosomia: (11x risk if birth weight >4Kg (5-23% for diabetics) 22x risk if birth weight >4.5 Kg (20-50% for diabetics)
- Maternal obesity
- Diabetes
- Postmaturity
- Precipitate delivery
- Advanced Maternal Age
- Male infants
- Excessive weight gain
- Previous macrosomia
- Previous shoulder dystocia
 "Dr Mike O'Connor") Author:Dr Mike O'Connor
Author:Dr Mike O'Connor| Tags:Shoulder Dystocia |