Low Dose Aspirin in the Prevention of Pre eclampsia and Fetal Growth Restriction
 "Low Dose Aspirin in the Prevention of Pre eclampsia and Fetal Growth Restriction")
Case Report
A 34-year-old primigravida presented with a fetal death in utero at 36+ weeks having had no fetal movements for 24 hours previously. Her blood pressure was then 140/100 and the protein/creatinine ratio was 144 mg/mmol. She had given the GP and obstetricians a strong family history of pre-eclampsia in her mother, sister and maternal aunt. Her blood pressure during pregnancy had been 100/65 at booking at 23-6 and had remained within normal limits until 36 weeks. Her urine had only been infrequently tested for proteinuria and her schedule of antenatal visits had not been as frequent as would even be normally expected: no visit between 31 weeks and 36 weeks. When the baby was delivered it weighed 1400g (<3rd percentile) and the placenta weighed only 258 g (<5th percentile).
Can Low Dose Aspirin Prevent This?
Preeclampsia is a complication of pregnancy secondary to placental dysfunction. Initially, vascular uterine re-modelling is altered, leading to decreased maternal blood supply to the placenta. Progressively, placental hypoxia and oxidative stress result in generalized dysfunction of the villous trophoblast. This placental dysfunction induces release into the maternal circulation of factors (free radicals, oxidized lipids, cytokines, sFlt-1) that cause generalized endothelial dysfunction, leading to clinical signs of the disease.
The first evidence of the obstetrical efficacy of aspirin was noted in 1985 by Beaufils et al., in a randomized study of preventive treatment with aspirin in 102 patients at high risk of preeclampsia and/or intrauterine growth restriction. The prevalence of preeclampsia was significantly reduced in the aspirin group compared with the untreated group (0/48 vs 6/45 p < 0.05).
The Place of Low Dose Aspirin as Primary Prevention of Pre Eclampsia
In 2001 Duley from Oxford and a team of Australian perinatologists including David Henderson-Smart, showed that low-dose aspirin (60-160 mg) reduced the risk of preeclampsia (PE) by 15% without changing the incidence of intrauterine growth restriction.
In 2007 a Cochrane Database study of a 37,000 patient meta-analysis found a 10% reduction in PE as well as a 10% reduction in deliveries before 34 weeks and a 10% reduction in perinatal morbidity and mortality. If aspirin was in doses >75 mg daily and commenced before 20 weeks the benefit was greater.
A further analysis suggested that there was no benefit from aspirin when the indication was nulliparity, chronic hypertension before pregnancy, diabetes before conception, age > 35 years, twin pregnancies, and history of a small-for-gestational-age infant.
Prevention of Intrauterine Fetal Growth Restriction with Aspirin
Bujold et al. found a risk reduction of 56% in patients at high risk when the treatment was started before 16 weeks of gestation (RR 0.44; 95% CI 0.30-0.65). After 16 weeks there was no benefit.
Screening For High Risk Factors for PE
Major Risk Factors
- Pre-eclampsia in previous pregnancy & birth <37 weeks or HELLP syndrome
-
Predisposing medical conditions Autoimmune eg
- Systemic Lupus erythematosus
- Scleroderma
- Anti-phospholipid syndrome
- Chronic hypertension (especially severe)
- Diabetes type 1 and 2
- Chronic kidney disease
- Assisted conception with oocyte donation
- Family history of pre-eclampsia (mother and/or sister)
For women with any major risk factor for pre-eclampsia, meta-analysis suggests a reduction in risk of pre-eclampsia of 46% (95% Cl 30% to 59%) when LDA therapy is initiated in early pregnancy. These women may also benefit from calcium. LDA will reduce the risk from about one in five to about one in ten in hgih risk women.
It is clearly important that all medical practitioners involved in antenatal care look for these risk factors so that low dose aspirin (+calcium) can be initiated well before 20 weeks and preferably before 16 weeks gestation.
Strategies for Detection of IUGR
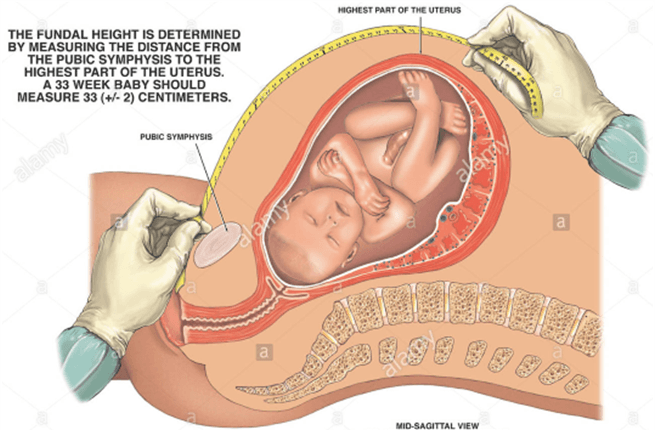
Fundal Symphyseal Height Measurements


There is a low sensitivity in late pregnancy (27%) and an 88% positive predictive value of fundal height measurements however poor measurement technique; maternal obesity; abnormal fetal lie, fibroids; polyhydramnios and engagement of the fetal head are confounding issues.
Ultrasound Assessment of Fetal Growth - the gold standard
The most sensitive indicator of symmetric and asymmetric IUGR is the abdominal circumference, which has a sensitivity of over 95 percent if the measurement is below the 2.5th percentile. Serial measurements are valuable as they will indicate a reduced velocity of growth.
Further Reading
Peleg D, Kennedy CM, Hunter SK. Intrauterine growth restriction: identification and management. Am Fam Physician 1998; 58: 453 460 and 466467.; Beaufils M, Donsimoni R, Uzan S, Colau JC. Prevention of pre-eclampsia by early antiplatelet therapy. The Lancet. 1985;325:840842. doi: 10.1016/S0140-6736(85)92207-X.
| Tags:UltrasoundMiscarriageObstetrcis |